Why does Vyvanse make me sleepy? Vyvanse makes you sleepy because of a phenomenon called paradoxical sedation — a well-documented response where the ADHD brain interprets dopamine regulation not as stimulation, but as permission to rest. Unlike the neurotypical brain, which experiences stimulants as energising, the ADHD brain that has spent years running in a state of hyperactivation can respond to dopamine normalisation with calm, settling — and even sleepiness. This is not a sign the medication is failing. In many cases, it is a sign it is working.

The Core Reason: Your ADHD Brain Is Wired Differently
The foundational explanation — and the one most patients aren’t told upfront — is that stimulants do not work the same way in ADHD brains as they do in neurotypical brains.
In a neurotypical brain, a stimulant produces an above-baseline surge of dopamine and norepinephrine that generates energy, hyperalertness, and arousal — the effect most people associate with “stimulants”. In an ADHD brain, the same stimulant brings dopamine levels from a chronically below-baseline state to a more functional level. The subjective experience of this correction is not stimulation — it is regulation: a quieting of the mental noise, a reduction in the hyperactive cognitive chatter, and a settling of the nervous system that can feel, to a brain unaccustomed to it, very much like sleepiness.
As one clinical summary puts it directly: “When the brain transitions from chaos to calm, it may interpret the shift as a signal to rest”. You are not actually tired in the physiological sense — your brain is experiencing a state of calm it has rarely or never had before, and it is misreading that calm as the onset of sleep.
The Brain Science: What’s Actually Happening When You Feel Sleepy
Understanding the neurochemical mechanism makes the experience less alarming and more actionable:
Chronic hyperactivation as a baseline:Many people with undiagnosed or undertreated ADHD spend years — sometimes decades — running on the neurological equivalent of having too many browser tabs open at maximum volume. The brain’s default mode network and executive function networks are in constant, poorly regulated flux. This is exhausting — but it is the only state the brain knows, so it has adapted to it. Adrenaline, cortisol, and deadline-driven activation have become the normal fuel source for getting through the day.
Vyvanse resolves the hyperactivation:When Vyvanse elevates dopamine in the prefrontal cortex, it restores the regulatory capacity that executive function requires. The background noise quiets. The hyperactive internal monologue slows. The frantic task-switching reduces. This is the therapeutic effect.
The brain misinterprets quiet as sleep:For a brain that has been in chronic hyperactivation, a state of genuine calm has no reference point except sleep. The shift is so unfamiliar that the nervous system responds as it would to a pre-sleep wind-down state — you feel drowsy, your eyes grow heavy, you may genuinely be able to fall asleep mid-morning. As patient communities consistently describe: “In an ADHD brain it causes relaxation — if it makes you feel sleepy and calm, it means that it is working”.
The Second Reason: Your Body Is Exhausted From Years of Unmanaged ADHD
This explanation is less discussed than the paradoxical sedation narrative but is, for many patients, equally or more relevant.
Living with unmanaged ADHD is cognitively and physically depleting. The constant effort of compensating for executive dysfunction — hyperfocusing to get things done, managing shame and frustration, maintaining the social performance that masks ADHD symptoms — is exhausting in a way that ADHD hyperactivity has been masking. The hyperactivity and adrenaline-driven coping mechanisms paradoxically keep people feeling functional even when they are deeply fatigued.
When Vyvanse regulates the executive function and reduces the hyperactive overdrive, that masking mechanism is removed. The fatigue that was always there — suppressed under years of compensatory hyperactivation — becomes visible. As one patient described: “If your body is too tired to function properly, but your ADHD is keeping you running anyway, stimulants will knock you out”.
This type of sleepiness is not a medication problem — it is the bill coming due for years of running on empty. The appropriate response is not to change the medication but to allow yourself to rest, reduce external demands where possible, and give your body the recovery it has been denied.
The Third Reason: Your Dose May Be Too High
When sleepiness occurs throughout the entire medicated window — not just in the first weeks of adjustment — it can be a signal that the dose is above your personal therapeutic ceiling:
- At too-high doses, the prefrontal cortex is pushed beyond its optimal operating range
- The result is a kind of neurochemical overwhelm that manifests as cognitive fatigue and sedation rather than enhanced focus
- This is distinct from the calm-calm of appropriate dosing — it has a heavy, foggy quality rather than a settled, clear quality
- The person can feel “switched off” rather than “switched on”
The dose-fatigue relationship is not linear. There is an inverted-U relationship between stimulant dose and cognitive performance: too low produces under-regulation (inattention, hyperactivity), the optimal range produces therapeutic regulation, and too high produces over-suppression (fatigue, emotional blunting, sedation).
As the clinical summary from HelloKlarity confirms: “Paradoxical sleepiness at a dose does not automatically mean the dose is too low. Some people need a lower dose, not a higher one”. This is one of the most important and most counterintuitive facts about Vyvanse sleepiness.
The Fourth Reason: Your Dose May Be Too Low
The opposite situation also produces sleepiness — though through a different mechanism and at a different time:
When the dose is too low, Vyvanse never reaches the therapeutic threshold for your individual neurochemistry. The ADHD is not meaningfully controlled, and the fatigue, cognitive slowing, and motivational collapse of undertreated ADHD persist throughout the day. This feels like sleepiness — but it is actually the ADHD itself, now slightly blunted but not resolved, producing the characteristic ADHD fatigue.
The distinguishing feature from too-high-dose sleepiness is the accompanying experience: at too-low doses, ADHD symptoms (distractibility, poor focus, task avoidance) are still clearly present alongside the tiredness. At too-high doses, ADHD symptoms may be controlled but accompanied by a heavy, suppressive drowsiness. The timing also differs — too-low-dose sleepiness tends to arrive early (4–6 hours) as the medication wears off prematurely; too-high-dose sleepiness tends to persist throughout the peak window.
The Fifth Reason: You’re Sleep-Deprived From the Night Before
One of the most practically important and most overlooked causes of daytime Vyvanse sleepiness is simple: the medication disrupted your sleep last night, and you are genuinely physically tired:
Vyvanse’s 10–14 hour active window means that a dose taken at 8 AM is still partially active at 8–10 PM. For patients with sleep onset sensitivity, this extends their time to fall asleep by 1–2 hours. For patients on higher doses, it can significantly fragment sleep architecture.
The accumulated sleep debt from this pattern means each morning begins on a compromised baseline. When the next dose of Vyvanse is taken, the brain — genuinely fatigued from inadequate sleep — responds to the medication’s regulatory effect by finally being able to rest rather than by engaging alert. The medication is working, but there is not enough neurological reserve to direct that work toward productivity rather than sleep.
This creates a compounding cycle: poor sleep → sleepy on Vyvanse → perception that medication isn’t working → dose may be escalated → further sleep disruption → worse fatigue → more sedation. Breaking the cycle requires addressing sleep first, before drawing conclusions about the dose.
How to Tell Which Reason Applies to You
The key diagnostic indicators:
| Your experience | Most likely cause |
|---|---|
| Sleepy in first 1–3 weeks, improving over time | Paradoxical sedation; adjustment period |
| Sleepy during peak window (3–8 hours), foggy quality | Dose too high |
| Sleepy and ADHD symptoms still present all day | Dose too low |
| Sleepy in first 1–2 hours, then awake by hour 3 | Onset adjustment; normal conversion curve |
| Sleepy after 8–10 hours, crashed feeling | Normal rebound; standard crash |
| Sleepy first thing in morning before medication kicks in | Sleep deprivation; prior-night sleep disruption |
| Deeply tired regardless of dose or timing | Burnout/underlying fatigue; investigate physical causes |
What to Do When Vyvanse Makes You Sleepy
Give It 2–3 Weeks First
For new patients, early-adjustment sleepiness is the most common type and the one most likely to resolve without any intervention. The brain adapts to the new neurochemical environment within 2–3 weeks, and the unfamiliar calm stops being misread as sleep. As one patient summarised: “It was gone after 2 weeks for me. And now after 4 months I feel just normal when meds work properly”. Do not escalate the dose or switch medications during the adjustment window — the sleepiness you’re experiencing may be the medication working correctly.
Optimise Sleep Before Evaluating the Dose
If you are experiencing daytime sleepiness, address sleep quality before concluding the medication needs adjustment:
- Take Vyvanse as early as possible after waking — ideally at or before 7–8 AM
- Create a consistent bedtime routine that begins 2–3 hours before sleep
- Avoid screens and stimulating activities in the 1–2 hours before bed
- If sleep onset is consistently more than 30–45 minutes, discuss low-dose melatonin (0.5–2 mg) with your prescriber
- Track your sleep hours — if you’re averaging under 7 hours, the sleepiness may be straightforward sleep deprivation interacting with the medication
Use Nutrition and Timing Strategically
- Eat before the medication begins to peak — taking Vyvanse on a completely empty stomach can intensify the sedating quality of the onset
- Stay hydrated — dehydration compounds cognitive fatigue and amplifies the sedated quality
- Avoid high-carbohydrate, low-protein morning meals — blood sugar spikes and crashes compound sleepiness
- Schedule your most demanding cognitive work during the peak window (hours 3–8), not during the onset or crash
Move Your Body at the Onset
Physical activity during the early onset window is one of the most reliably reported strategies for converting Vyvanse’s calming effect into productive focus rather than drowsiness:
- A 20–30 minute brisk walk or light exercise session taken 1–2 hours after dosing helps direct the activated neurochemistry toward wakefulness rather than sedation
- Exercise independently elevates dopamine and norepinephrine — working synergistically with Vyvanse rather than against it
Talk to Your Prescriber About the Pattern
If sleepiness persists beyond 3 weeks, is occurring throughout your entire peak window, or is severe enough to interfere with daily function:
- Document the timing precisely — when the sleepiness begins, how long it lasts, what quality it has (heavy and foggy vs. calm and clear)
- Report whether ADHD symptoms are well-controlled or still present — this helps distinguish too-high from too-low dosing
- Describe your sleep — hours, quality, difficulty falling asleep
- Your prescriber can assess whether a dose reduction, upward adjustment, timing change, or different medication is indicated
Safety and Important Considerations for Australian Adults
- Extreme drowsiness from the very first dose — before any adjustment period — is a potential paradoxical reaction that warrants immediate prescriber contact before continuing. This is distinct from the common mild early-adjustment sleepiness
- Do not drive or operate machinery if Vyvanse is making you significantly drowsy — despite being a stimulant, sedation severe enough to impair reaction time is a genuine risk during the adjustment phase or if the dose is too high
- Sleepiness that arrives alongside emotional blunting, persistent low mood, or lack of motivation should be reported promptly — these are signs of over-suppression that require prescriber review rather than patient management
- Sleep apnoea is significantly more common in the ADHD population than in the general population and is frequently undiagnosed. If you are sleepy despite adequate sleep hours, and particularly if you snore or wake unrefreshed, discuss a sleep study with your GP before attributing the fatigue exclusively to Vyvanse
Common Misconceptions About Vyvanse and Sleepiness
Myth 1: “Vyvanse making me sleepy means I don’t have ADHD.”The paradoxical sedation response is actually more characteristic of the ADHD brain than the non-ADHD brain. Neurotypical individuals taking stimulants typically experience increased energy and arousal; ADHD individuals experience regulation and calm. Feeling sleepy on Vyvanse is — in the adjustment context — broadly consistent with the ADHD diagnosis, not contrary to it.
Myth 2: “I need a higher dose if the medication is making me sleepy.”This is the most important misconception to resist. Sleepiness during the peak window specifically can be a sign the dose is already too high. Escalating the dose in this scenario worsens the sedation. Timing is the essential diagnostic: sleepiness during the peak window → consider dose reduction; sleepiness only during the early crash → consider dose increase or timing change.
Myth 3: “Once Vyvanse makes you sleepy, it will always make you sleepy.”Adjustment-phase paradoxical sedation resolves for the majority of patients within 2–3 weeks. The sleepiness is a feature of the initial neurochemical shift, not a permanent pharmacological property of Vyvanse at your dose. Many patients who found the first two weeks severely soporific report complete resolution and normal therapeutic function thereafter.
Myth 4: “If the medication makes me sleepy, it isn’t doing anything.”Feeling calmer, quieter, and less chaotically hyperactive is the mechanism by which Vyvanse treats ADHD — and that state, unfamiliar to a brain that has never experienced it, feels like sleepiness. The medication is doing something; the brain is interpreting it incorrectly because it has no prior reference point for this kind of regulatory calm.
Why does Vyvanse make me sleepy Hobart
Why does Vyvanse make me sleepy Devonport
Why does Vyvanse make me sleepy Launceston
Why does Vyvanse make me sleepy Tasmania
Why does Vyvanse make me sleepy Victoria
Why does Vyvanse make me sleepy Queensland
Why does Vyvanse make me sleepy Canberra
Why does Vyvanse make me sleepy Australian Capital Territory
Why does Vyvanse make me sleepy South Australia
Why does Vyvanse make me sleepy New South Wales
Why does Vyvanse make me sleepy Darwin
Why does Vyvanse make me sleepy Ghan
Why does Vyvanse make me sleepy Northern Territory
Why does Vyvanse make me sleepy Australia
Why does Vyvanse make me sleepy Austria
Why does Vyvanse make me sleepy Germany
Why does Vyvanse make me sleepy United Kingdom
Why does Vyvanse make me sleepy Sweden
Why does Vyvanse make me sleepy Denmark
Why does Vyvanse make me sleepy Norway
Why does Vyvanse make me sleepy Finland
Why does Vyvanse make me sleepy Iceland
Why does Vyvanse make me sleepy Netherlands
Why does Vyvanse make me sleepy Spain
Why does Vyvanse make me sleepy Ireland
Why does Vyvanse make me sleepy Switzerland
FAQ: People Also Ask About Vyvanse and Sleepiness
Is it normal for Vyvanse to make you sleepy?Yes — it is a recognised and common experience, particularly in the first weeks of treatment. Between 20–30% of ADHD patients experience some degree of fatigue or sedation on stimulant medications, and in many cases this reflects the paradoxical regulatory response of the ADHD brain rather than a problem with the medication. Most cases resolve within 2–3 weeks; persistent sleepiness at a stable dose warrants prescriber review.
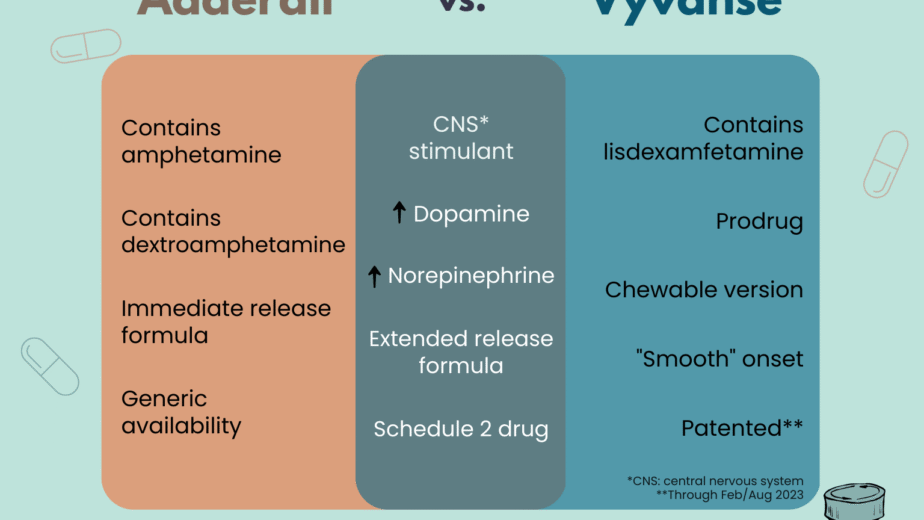
Why does Vyvanse make me sleepy but Adderall didn’t?Vyvanse’s prodrug mechanism produces a slower, lower-peak dextroamphetamine onset compared to immediate-release amphetamines like Adderall. This gentler, more sustained rise produces less of the sharp alerting quality that immediate-release formulations deliver. The calming, regulatory quality of Vyvanse is more pronounced than the stimulating quality — which is clinically beneficial but experientially more likely to produce sedation in patients whose ADHD brain interprets dopamine regulation as a signal to rest.
How long does the sleepiness from Vyvanse last?Adjustment-phase sleepiness typically resolves within 2–3 weeks as the brain adapts. If it has not resolved within 3–4 weeks at a stable dose, it is less likely to be adjustment-related and more likely to reflect dose, timing, or sleep quality issues that require clinical management.
Does Vyvanse sleepiness mean the dose is wrong?Not necessarily, and not always in the direction you’d expect. Paradoxical sedation during adjustment is not a dosing problem at all — it is a neurological adaptation process. If sleepiness persists, it may mean the dose is too high (most common for sleepiness during the peak window) or too low (most common for early-crash tiredness with persisting ADHD symptoms). The pattern of when the sleepiness occurs is the most important clinical indicator.
Can I drink coffee to counteract Vyvanse sleepiness?Caffeine is not recommended as a routine solution to Vyvanse sleepiness. It compounds cardiovascular stimulation, worsens anxiety, and — most significantly — disrupts sleep, which perpetuates the sleep deprivation that may be causing or worsening the daytime drowsiness. If caffeine is helping significantly with Vyvanse-related sleepiness, this is a signal to discuss the dose and timing with your prescriber rather than to continue relying on caffeine as a compensatory tool.
Should I tell my doctor that Vyvanse makes me sleepy?Yes — always. Your prescriber needs to know whether the medication is producing the intended therapeutic effect or an adverse sedating effect. The distinction between adjustment-phase sedation (normal, likely to resolve), dose-too-high sedation (requires reduction), and dose-too-low fatigue (requires adjustment upward) cannot be made without the specific timing and quality information only you can provide. Bring precise notes: when the sleepiness begins, how long it lasts, whether ADHD symptoms are well-controlled, and your sleep quality the prior night. This information is clinically essential.